what can you do to relieve the pain of cervical radiculopathy that is compressing the ulnar nerve
Original Editor - Stéphanie Dartevelle
Top Contributors - Scott Buxton, Admin, Jasper Vermeersch, Stéphanie Dartevelle, Rachael Lowe, Kim Jackson, Garima Gedamkar, Scott Cornish, Simisola Ajeyalemi, Thomas Rodeghero, Jesse Demeester, Laura Ritchie, WikiSysop, Evan Thomas, Stijn De Coninck, Venugopal Pawar, Fasuba Ayobami, Maxime Tuerlinckx, Candace Goh, Rucha Gadgil, Wendy Walker, Khloud Shreif, Olajumoke Ogunleye, Johnathan Fahrner and Jelle Van Hemelryck
Definition/Description [edit | edit source]
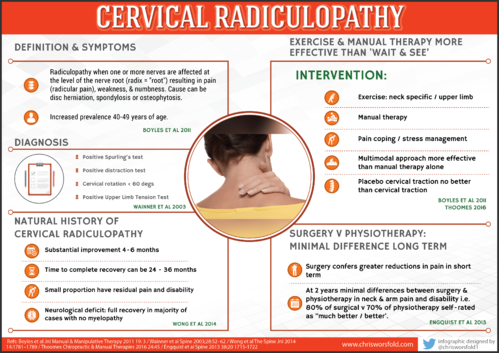
"Cervical radiculopathy is a disease process marked by nerve compression from herniated disk material or arthritic bone spurs. This impingement typically produces cervix and radiating arm pain or numbness, sensory deficits, or motor dysfunction in the neck and upper extremities."[1]
Cervical radiculopathy occurs with pathologies that cause symptoms on the nervus roots. [ii] Those can exist compression, irritation, traction, and a lesion on the nerve root acquired by either a herniated disc, foraminal narrowing, or degenerative spondylitic change (Osteoarthritic changed or degeneration) leading to stenosis of the intervertebral foramen[ii][3].
Most of the time cervical radiculopathy appears unilaterally, however information technology is possible for bilateral symptoms to be present if severe bony spurs are present at one level, impinging/irritating the nerve root on both sides. If peripheral radiation of pain, weakness, or pins and needle are present, the location of the pain will follow back to the concerned affected nerve root[2]
Clinically Relevant Anatomy [edit | edit source]
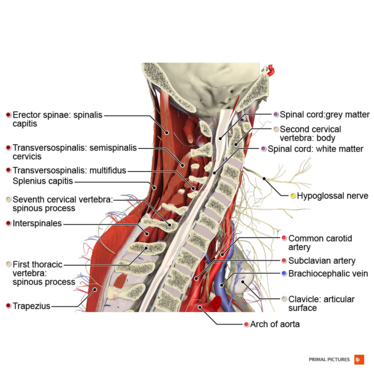
The homo body has 8 cervical nervus roots, for 7 cervical vertebrae and this may seem confusing at first. Nonetheless a nerve root comes out of the spinal column betwixt C7 and T1, hence C8 as T1 already exists [two] . Tanaka Northward. et al[4] used a surgical microscope to practise an anatomic study of the cervical intervertebral foramina, nerve roots, and intradural rootlets. The intervertebral foramina were shaped like a funnel with the entrance zone being the most narrow part. This was considered the place where the pinch of the nerve roots in the intervertebral foramina occurs. Compression of the roots at the inductive side was ascribed to protruding discs and osteophytes of the uncovertebral region. Compression on the posterior side was acquired past the superior articular process, the ligamentum flavum, and the periradicular gristly tissues.
Nerve roots and the local vessels lack a perineurium and accept a poorly developed epineurium, making them vulnerable to mechanical injury when compared to the periphery. The blood supply is besides less secured and vulnerable to ischemic damage[five]. These anatomical differences to peripheral nerves may explain why depression pressures on the nerve root elicit large changes and signs and symptoms. The nerve roots are vulnerable to pressure damage which is why small impingements can cause signs and symptoms.
At 5-10mmHg (0.1psi) capillary stasis and ischemia has been observed with partial blockage of axonal transport. At 50mmhg tissue permeability increases with an influx of oedema, college than 75mmhg, there is nervus conduction failure if sustained for 2 hours. At lxx+mmHg neural ischemia is complete and conduction is not possible[5]. It is rare to get pressures that high only v-10mmhg is a big small amount of pressure and signs and symptoms occur[5]. These pressures can occur with a less severe clinical flick in unique circumstances, if the pressure is acute so symptoms are astringent however if chronic the nervous tissue is given fourth dimension to adjust and evolve to the surrounding structure and symptoms are less astringent.
Epidemiology / Etiology [edit | edit source]
Cervical radiculopathy is a dysfunction of a nerve root in the cervical spine, is a wide disorder with several mechanisms of pathology and it can affect people of any age, [6] with meridian prominence between the ages of 40-50 [2] [vii] [8]. Reported prevalence is 83 people per 100,000 people [8]. Annual incidence has been reported to be 107,iii per 100.000 for men and 63,v per 100.000 for women[9] [x].
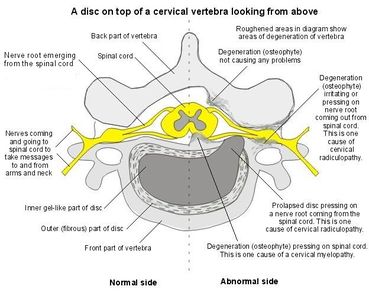
Basic Moving-picture show of a Cervical Vertebral Torso
The 2 main mechanisms of the nerve root irritation or impingement are: [9]
- Spondylosis leading to stenosis or bony spurs - more than common in older patients
- Disc herniation - more common in younger patients
Mechanical pinch from spondylosis can impact the neuroforamen from all directions, which limits nerve root excursion. Cytokines released from damaged intervertebral discs can too cause this disorder. [9]
There is increasing evidence that inflammation itself and/or in association with root compression is the principal cause of symptoms and signs. This is proved by the presence of interleukins and prostaglandin in herniated discs and the spontaneous recovery within weeks or months in the majority of patients.[11]
The about mutual level of root compression is C7 (reported percentages 46.3–69%), followed by C6 (19–17.6%); compression of roots C5 (ii–half dozen.vi%), and C8 (10– 6.2%) are less frequent. I possible explanation is that intervertebral foramina are largest in the upper cervical region and progressively decrease in size in the eye and lower cervical areas, with an exception of the C7-Th1 foramen (C8).[11] [12]
Characteristics/Clinical Presentation [edit | edit source]
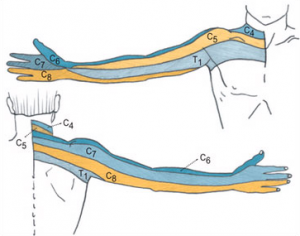
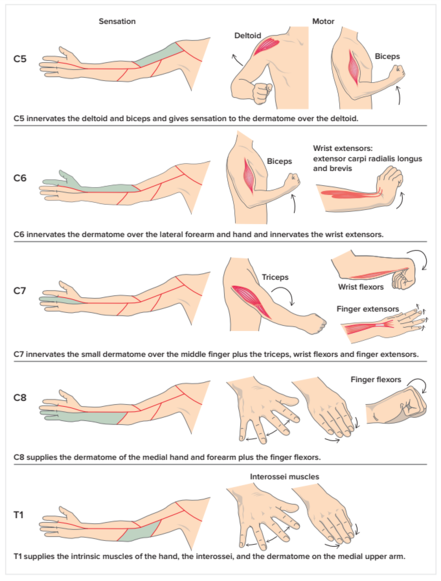
Typical Dermatomal Pattern of the Upper Limb
Typical symptoms of cervical radiculopathy are: irradiating arm pain corresponding to a dermatomal pattern, neck hurting, parasthesia, musculus weakness in a myotomal pattern, reflex damage/loss, headaches, scapular pain, sensory and motor dysfunctionin upper extremities and neck[2] [6] [3] [13] [xiv].
Upper limb movements that are affected:
- C1/C2- Neck flexion/extension
- C3- Neck lateral flexion
- C4- Shoulder meridian
- C5- Shoulder abduction
- C6- Elbow flexion/wrist extension
- C7- Elbow extension/wrist flexion
- C8- Pollex extension
- T1- Finger abduction
The absenteeism of radiating pain does non exclude nerve root compression. The aforementioned appears with sensory and motor dysfunction that might be present without significant pain [two].
Symptoms are generally amplified with movements that may be unidirectional or multidirectional reduce the infinite available for the nerve root to get out the foramen causing impingement [2]. This frequently causes the patient to present with a stiff cervix and a subtract in cervical spine ROM, secondary musculoskeletal bug, decrease in muscle length of the cervical spine musculature (upper fibres of trapezius, scaleni, levator scapulae), weakness, articulation stiffness, capsule tightness, and postural defects which tin can continue to touch on movement mechanisms of the rest of the body.
Differential Diagnosis [edit | edit source]
Differentiating from cervical radiculopathy is derived from a combination of a patient's history, physical examination, and radiological findings. [15] Pathologies which mimic the signs and symptoms of radiculopathy.[16]
- Spinal Tumor
- Systemic diseases known to cause peripheral neuropathies
- Cervical myelopathy
- Ligamentous Instability
- Vertebrobasilar Insufficiency (VBI)
- Shoulder Pathology
- Peripheral nerve disorders
- Thoracic outlet syndrome
- Brachial plexus pathology
- Systemic affliction
- Parsonage-Turner syndrome
- Superior pulmonary sulcus tumour
Diagnostic Procedures [edit | edit source]
The nigh common diagnostic methods used to assess the presence of possible compression are radiographs, MRI and electrophysiologic studies (EMG + Nerve Conduction Studies) to examine the nerve root and nerve conduction velocity [17] [2] [6].
Root compression seen on an MRI may confirm cervical radiculopathy, but to find foraminal stenosis, which causes a bony compression on the nervus, screw CT is described as the best manner to observe this.[11]
There even so is no consensus on whether conventional needle myography (EMG) has a stiff diagnostic value for cervical radiculopathy. Several unblinded studies have reported sensitivities ranging from thirty-95%.[11]
A subjective history and mechanism of Injury can be integral to an authentic diagnosis and the crusade of radiating arm hurting. More frequently acute radiating arm pain is caused by a disk herniation, while chronic bilateral axial neck and radiating arm hurting is usually acquired by cervical spondylosis [two].
Issue Measures [edit | edit source]
Neck disability alphabetize NDIPatient Specific Functional Scale PSFS
Numerical Hurting Rating Scale NPRS
Cervix Hurting and Inability Scale (NPAD)
Examination [edit | edit source]
Provocative tests are performed to provoke or worsen the symptoms in the affected arm and are indicative of cervical radiculopathy.[11]
Wainner et afifty[18] examined the accuracy of the clinical examination and adult a clinical prediction dominion to aid in the diagnosis of cervical radiculopathy. Their inquiry demonstrated that these 4 clinical tests, when combined, hold high diagnostic accuracy compared to EMG studies:
- Spurlings Test,
- Upper limb tension-i
- Distraction examination
- involved side cervical rotation range of movement less than 60 degrees.
When all 4 of these clinical features are present, the post examination probability of cervical radiculopathy is 90%, Where but 3 of the 4tests are positive the probability decreases to65%[18] [iii] [6] [19]. A further combination of tests with good reliability are the combination of Spurlings Examination, Cervix Distraction, Valsalva and Upper Limb Tension Tests 1, 2aand 2b [xx] .
Tong HC et al [21] . performed the Spurling test before imaging was completed. The test had a sensitivity of 30% and a specificity of 93%. They concluded that the Spurling test is not sensitive, merely it is very specific for cervical radiculopathy. It is therefore not useful as a screening test but it tin well exist used to confirm a cervical radiculopathy.
A report conducted past Gumina et al[22] found Arm Squeeze test useful to distinguish betwixt cervical nerve root compression and shoulder disease. The test has 96% for both sensitivity and specificity, inter-observer value of 0.81 and intra-observer value of 0.87. Nevertheless, the exam utilizes subjective measures and needs to exist validated.
The neurologic examination has moderately stiff intraobserver reliability with a kappa value between 0.iv and 0.64 The sensory exam can distinguish betwixt a C8 radiculopathy and ulnar neuropathy, as at that place will be splitting of the hyperalgesia in either the third or fourth digit with ulnar neuropathy. With C8 radiculopathy, the unabridged digit will be affected. Motor examination may or may not prove a grade of weakness in the myotome that corresponds to the pathologic nerve. No myotome corresponds to the upper iv cervical nerve roots. C5 radiculopathy may show weakness in the deltoids (evaluated past testing for shoulder abduction); C6 will evidence weakness in the biceps and flexor carpi ulnaris (evaluated past testing for wrist extension); C7 weakness occurs in the triceps, besides as the brachioradialis (evaluated by testing for ellbow extension); C8 pathology causes weakness in the intrinsic muscles of the paw, equally evaluated by finger abduction and grip. Muscle stretch reflexes also tend to be decreased in the setting of radiculopathy. Biceps hyporeflexia is indicative of C6 radiculopathy, while decrease in the triceps and brachioradialis reflexes corresponds to pathology at C7. co-ordinate to Viikari-Juntura(1989).[23] [24]
Medical Management [edit | edit source]
There are several intervention strategies for managing cervical radiculopathy, with physical therapy and surgical interventions existence the most common. The long term benefits of surgical interventions are questionable all the same with 25% of patients continuing to experience pain and disability at 12 calendar month follow-ups [25]. At that place is a pregnant corporeality of evidence to back up the apply of physical therapy interventions [26], and the benefit of physical therapy and manual techniques in general for patients with cervix hurting with or without radicular symptoms.
Surgery [edit | edit source]
Indications for a single level surgery; [27]:
- Sensory symptoms (radicular pain and/or paresthesias) in a dermatomal distribution that correlates with involved cervical level
- Motor deficit, reflex changes or positive EMG correlated to involved cervical level
- A positive response to a selective nerve root cake (SNRB).
- Positive MRI or myelogram with computed tomography (CT) scan.
- At least half-dozen weeks of conservative care such as physical therapy, epidural injections, NSAID'due south, pain killers.
- In instance of clear motor deficit, 6 weeks of bourgeois care are not required.
Criteria for a 2nd level surgery:
- All of the criteria previously described for a single level surgery, not including SNRB, are nowadays at the chief level.
- The adjacent level has radicular pain correlating with at least moderate foraminal stenosis or lateral recess herniation or EMG changes, motor deficits or reflex changes correlated to adjacent level.
Operative techniques that are frequently used equally handling for cervical radiculopathy are:
- Anterior Cervical Dissectomy (decompression) (ACD),
- Anterior Cervical Dissectomy and Fusion (ACDF),
- Total Disc Arthroplasty (TDA),
- Laminotomy,
- Foraminotomy,
- Corpectomy.[28] [27]
Engquist M et al. found that surgery with physiotherapy resulted in a more rapid improvement during the first postoperative year, with significantly greater improvement in neck pain and the patient's global assessment than physiotherapy solitary. The differences between the groups decreased afterward 2 years. They suggested that structured physiotherapy should be tried before surgery is called.[29]
Persson et al. concluded that there were no long term (i yr) differences between surgery and physical therapy in strength, pain and sensation. Several other studies demonstrated that physical and social operation and pain significantly improved afterward surgery, although these improvements remained relatively short termed (max ane year) and diminished after a longer catamenia (1 to 4 years).[28]
ACDF is associated with diminished ROM and strength compared to conservative treated subjects. This can, occasionally, be associated with prolonged hurting.[28]
Peolsson A et al. concluded that ACDF did not result in boosted improvements in neck agile range of motility, neck muscle endurance, or hand-related role compared with a structured physiotherapy program alone in patients with cervical radiculopathy. The commodity suggests that a structured physiotherapy plan should precede a determination for ACDF intervention in patients with cervical radiculopathy, to reduce the need for surgery.[31]
Short duration of hurting, low health quality, high levels of anxiety due to neck/arm pain, low cocky-efficacy, and a high level of distress before treatment were associated with poor outcomes from surgery.[29]
Injections [edit | edit source]
Epidural steroid injections tin can likewise be used as treatment for cervical radiculopathy. The injections are given under the guidance of fluoroscopy or CT. There is limited show that transforaminal epidural steroid injections provide relief for sixty% of the patients and about 25% of the patients with clear surgical indications. Steroid injections are non a causal handling and are not a solution, although they tin can be considered when developing a medical/interventional treatment plan for patients with cervical radiculopathy from degenerative disorders. Trans-foraminal injections are not without risk and possible complications such as spinal cord injury and death must be considered before performing this procedure.[32] [33]
Lee SH et al. researched the use of ESI (Epidural Steroid Injections) in patients diagnosed with cervical soft disc or difficult disc causing nerve root compression and symptoms. In more than eighty% of patients with CR who were surgical candidates, surgery was avoided using ESI. The significant factors predisposing failure of ESI were intensity of symptoms and a previous episode of CR. [34]
Physical Therapy Direction [edit | edit source]
Although a definitive treatment progression for treating cervical radiculopathy has not been adult, a general consensus exists within the literature that using manual therapy techniques in conjunction with therapeutic exercise is constructive in regard to increasing part, every bit well as agile range of motion (AROM), focusing on decreasing levels of pain and disability will most likely be the main focus of the patient [35]. Recent high level research confirms the positive outcomes of do therapy[26].
If the patient has had long-term hurting, an element of hurting sensitisation may have developed and chronic hurting behaves differently to acute hurting. Therefore educational activity virtually pain and reconceptualisation may be necessary.
Treatment Options:
- Education and advice
- Transmission Therapy - PAIVMs (Passive Assessory Intervertebral Movements) / PPIVMs (Passive Physiological Intervertebral Movements) / NAGs (Natural Apophyseal Glides) / SNAGs (Sustained Natural Apophyseal Glides)
- Exercise Therapy - AROM, stretching and strengthening
- Postural re-education
Education and Advice [edit | edit source]
Education is key to getting the patient on side and to work co-operatively with physiotherapy. If a patient understands the condition and the reason for the neck and arm pain then they are more likely to be compliant with any rehabilitation programme.
In cases of a prolapsed disc, tobacco smoking causes constriction of the vascular network surrounding the intevertebral disc (IVD), reducing the indirect exchange of nutrients and anabolic agents from the blood vessels to the disc. Nicotine down-regulates the proliferation rate and glycosaminoglycan (GAG) biosynthesis of disc cells. Nicotine by and large affects the GAG concentration at the cartilage endplate, reducing it upwards to 65% of the value attained in normal physiological weather condition. Tabacco mostly affects the nucleus pulposus, whose cell density and GAG levels reduce upwards to 50% of their normal physiological levels. The effectiveness of quitting smoking on the regeneration of a degenerated IVD shows limited benefit on the wellness of the disc. Jail cell-based therapy in conjunction with fume cessation should provide significant improvements in disc health, suggesting that, too quitting smoking, boosted treatments should be implemented in the attempt to recover the health of an IVD degenerated by tobacco smoking.[36]
Manual Therapy [edit | edit source]
In that location are some contradictions for using manual therapy techniques and its efficacy is questioned. Gross AR et al reported mobilisation and/or manipulation when combined with exercise was benign for pain relief and comeback of office for persistent mechanical neck disorders with or without headache, but as a stand alone treatment manipulation and/or mobilisation was not benign. This is echoed in the electric current literature. In a multimodal treatment model, the addition of manual therapy techniques (thought to increase the size of the intervertebral foramen of the affected nerve root) has no pregnant additional benefits [37] [38] [39] Compared to ane another, neither was superior either.[xl] At all-time manipulations may likewise but provide short term pain relief [41]
Furthermore, cervical spine manipulation carries a adventure of complications like vertebral dissection and spinal cord compression because of massive disc herniation. Therefore, this intervention should be discouraged in cervical radiculopathy, especially if imaging of the spine has not nonetheless been performed.[11] Aware of any potential adventure factors such as arterial insufficiency, Hypertension, Craniovertebral ligament insufficiency and upper motor neurone disorders is also essential[42].
Fritz JM et al examined the effectiveness of cervical traction in addition to practise in patients with cervical radiculopathy. Adding mechanical traction to practice for patients with cervical radiculopathy resulted in lower inability and pain, particularly at long-term follow-ups.[43] [44]
Boyles et al (2011) [45] nonetheless found that manual therapy consisting of thrust mobilisations of the cervical or thoracic spine and cervical not-thrust mobilisations (PA glides/Lateral Glides in ULTT1 position/Rotations/Retractions) was shown to exist effective at reducing hurting levels, improving function and increasing joint ROM. When combined with exercise therapy information technology was more than effective than the control group of manual therapy or do therapy still both control groups were effective at reducing signs and symptoms[46].
Persson et al highlighted that there was no significant difference between event measures of patients who had had surgery, physiotherapy or cervical collar explaining that physiotherapy is at to the lowest degree as effective as surgery.
Muscle Energy Techniques [edit | edit source]
Cleland et al [47] utilised musculus energy techniques (MET) in 28 patients, 46% receiving positive outcomes. Yet details of the techniques used were insufficient and a variety of techniques were used every bit information technology was down to the practitioner to decide which technique would be used.
The quality of inquiry related to testing the effectiveness of MET is poor. Studies are generally small and at high risk of bias due to methodological deficiencies.[48]
Neurodynamics - Gliding and Sliding/Tensioning [edit | edit source]
Ragonese (2009)[46] performed the neurodynamics sliding and tensioning techniques, outlined by Butler [49], whilst having the patient in an upper limb tension positions described by Magee[50] conducted in a tiresome and oscillatory manner. With improvement in symptoms, the technique was progressed to a 'tension' technique, also described past Butler. Again, positive outcomes were observed in regards to pain and function, although treatment duration was not recorded.
Exercise Therapy [edit | edit source]
Practice therapy has the most positive and lasting furnishings for the condition.[26] Exercises targeted at opening the intervertebral foramen are the best pick for reducing the impact of radiculopathy. Exercises such as contralateral rotation and sideflexion are amid the simplest forms of exercises which are effective confronting signs and symptons, given in the form of active ROM[37]. Due to the intricate and shut relationship of muscles on the intervertebral foramen and the likely presentation of reduced ROM, stretching is besides an effective form of treatment to regain ROM[51]
Once ROM increases strengthening exercises tin can exist performed to develop stability and reduce the risk of developing nerve root irritation in the future, as long as it is not caused by a structure which cannot be influenced past physical therapy. During the initial stages of treatment, strengthening should be limited to isometric exercises in the involved upper limb. Once the radicular symptoms accept been resolved, progressive isotonic strengthening can brainstorm. This should initially involve low weight and high repetitions (15-xx repetitions). Airtight kinetic concatenation activities tin can be very helpful in rehabilitating weak shoulder girdle muscles. However, Griffiths et al plant no significant departure with the addition of specific neck stabilisation exercises to a programme of general cervix communication and do [52].
Patient should be instructed to remain every bit active as possible and perform exercises daily on the days between therapy sessions. Written exercise instructions should therefore be available. We propose a two components program, every bit suggested past Fritz JM et al. 2 components: scapula strengthening and cervical strengthening.
Cervical strengthening exercises should include supine craniocervical flexion to elicit contraction of the deep neck flexor muscles without contraction of superficial neck muscles [53]. Feedback using an air-filled pressure level sensor or tactile cues tin be useful. Patient should perform three sets of 10 contractions of ten seconds with proper muscle activation. Craniocervical flexion contractions were likewise performed with the patient seated, with the goal of 30 repetitions of 10-second contractions.
Scapular retraction against resistance using elastic bands or pulleys can be added. Scapular-strengthening exercises included decumbent horizontal abduction, sidelying forward flexion, prone extension of each shoulder, as well as decumbent push-ups with emphasis on shoulder protraction. The goal was iii sets of x repetitions, with resistance added as tolerated.
Prognosis [edit | edit source]
Regarding physical therapy interventions, in 2007 Joshua Cleland and colleagues[47] examined the predictors of positive short-term outcomes in people with a clinical diagnosis of cervical radiculopathy. The following clinical features were plant to be about predictive of a positive short-term issue:
- Age <54
- Dominant arm not affected
- Looking downwardly does not worsen symptoms
- Handling involves manual therapy, cervical traction, and deep neck flexor strengthening for at least 50% of visits
If 3 of these features are present, the probability of success is 85%, and increases to xc% if all four are present[54]
Clinical Bottom Line [edit | edit source]
Cervical radiculopathy is defined equally a disorder (pinch, traction, irritation, herniated disk) affecting a spinal nerve root in the cervical Spine. Cervical radiculopathy typically produces cervix and radiating arm hurting, numbness, sensory deficits, or motor dysfunction in the neck and upper extremities. Information technology is important to have knowledge of the cervical anatomy, considering it is the key to constructive physiotherapy practice and treatment.
Because there are other pathologies that have the same signs and symptoms of radiculopathy, it'southward recommended to practise a good examination. You can use imaging studies (MRI) or electro physiologic studies(EMG + Nerve Conduction Studies) [55] [1] [38]. Meliorate, is to use these 4 clinical tests: Spurlings Test, Upper limb tension-ane Distraction examination and Cervical Flexion Rotation Test. When all 4 of these clinical test are positive, the post-exam probability of cervical radiculopathy is xc%.
The main focus for concrete therapy or medical direction of cervical radiculopathy, is decreasing the hurting and disability. Once the treatment is started, it's important to choose the right tool to evaluate your patient. The Neck disability index is a good option.
References [edit | edit source]
- ↑ 1.0 1.ane Eubanks J. Cervical Radiculopathy: Nonoperative Management of Neck Hurting and Radicular Symptoms. Am Fam Medico. 2010 Jan i;81(ane):33-forty.
- ↑ 2.0 2.1 ii.ii 2.three 2.four 2.five two.6 2.7 2.eight 2.ix Eubanks, JD.Cervical Radiculopathy:Nonoperative Management of Cervix Pain and Radicular Symptoms.American Family Dr. 2010;81,33-40
- ↑ 3.0 3.1 iii.2 Kenneth A. Olson. Manual physical therapy of the spine.Saunders Elsevier 2009.p 253, 257, 258
- ↑ Tanaka N. et al, The anatomic relation among the nerve roots, intervertebral foramina, and intervertebral discs ofthe cervical spine. Spine. 2000 February; 25(3): 286-291
- ↑ five.0 5.ane five.2 Lipetz, JS. Pathophysiology of inflammatory, degenerative, and compressive radiculopathies. Phys Med Rehabil Clin N Am. 2002. thirteen: 439–449
- ↑ 6.0 6.1 half-dozen.2 6.three Young IA,Michener LA,Cleland JA,Aguilera AJ,Snyder AR.Manual therapy, exercise, and traction for patients with cervical radiculopathy: a randomize clinical trial.Physical Therapy 2009;89:632-642
- ↑ Radhakrishnan Thousand, Litchy WJ, O'Fallon 1000, et al. Epidemiology of cervical radiculopathy: A population-based study from Rochester, Minnesota, 1976 through 1990. Encephalon 1994; 117:325-335.
- ↑ 8.0 viii.one Bogduk N. Twomey CT. Clinically Relevant Beefcake for the Lumbar Spine. 2ed. Edinburgh UK: Churchill Livingston. 1991
- ↑ 9.0 9.1 9.2 Barrett I. et al. Cervical Radiculopathy Epidemiology, Etiology, Diagnosis, and Treatment. Periodical of Spinal Disorders &Techniques. April 2015; 28:five.
- ↑ Radhaknshnank et al. Epidemiology of Cervical Radiculopathy. A Population Based Written report. Brain. 1994: 117; 325-335
- ↑ 11.0 eleven.1 11.2 11.3 xi.4 xi.5 Kuijper B. et al. Degenerative cervical radiculopathy: diagnosis and conservative treatment: A review. European journal of neurology. 2009; 16(1): fifteen-20
- ↑ Ellenberg M, Honet J, Treanor Westward. Cervical Radiculopathy. Arch Phys Med Rehabil. 1994; 75:342-352.
- ↑ Kenneth W. Lindsay, Ian Bone.Neurology and neurosurgery illustrated.4th ed. Churchill Livingstone.p408
- ↑ Kuijper B, Tans JT, Beelen A, Nollet F, de Visser M.Cervical collar or physiotherapy versus look and encounter policy for recent onset cervical radiculopathy : randomised trial.BMJ 2009;p1-seven
- ↑ Gu R., et al. Differential diagnosis of cervical radiculopathy and superior pulmonary sulcus tumor. Chinese medical periodical. 2012 August; 125(15): 2755-2757
- ↑ C: R. Erhard et al. Cervical Radiculopathy or Parsonage-Turner Syndrome: Differential Diagnosis of a Patient With Cervix and Upper Extremity Symptoms. JOSPT. October 2005fckLRVolume 35, No. 10
- ↑ Partanen J, Partanen K, Oikarinen H, et al. Preoperative electroneuromyography and myelography in cervical root compression. Electromyogr Clin Neurophysiol. 1991; 31:21-26.
- ↑ 18.0 18.1 Wainner RS, Fritz JM, Irrgang JJ, et al. Reliability and diagnostic accuracy of the clinical examination and patient cocky-report measures for cervical radiculopathy. Spine. 2003;28(1):52-62.
- ↑ C: Wainner et al. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003 Jan one. 28(1):52-62.
- ↑ Sidney M. et al. A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy. European Spine Periodical. April 2006; 16(3): 307-319 LoE: 2A
- ↑ Tong HC, Haig AJ, Yamakawa K.. The spurling examination and cervical radiculopathy. Spine. 2002 Jan;27(2):156-159. LoE: 2B
- ↑ Gumina, S., Carbone, S., Albino, P., Gurzi, M., & Postacchini, F. (2013). Arm Squeeze Test: a new clinical test to distinguish cervix from shoulder pain.European Spine Journal,22(7), 1558–1563. http://doi.org/10.1007/s00586-013-2788-3
- ↑ Viikari-Juntura E, Porras One thousand, Laasonen EM. Validity of clinical tests in the diagnosis of root compression in cervical disc affliction. Spine (Phila Pa 1976) 1989;fourteen(three):253–257. LoE: 2B
- ↑ John M. Caridi. Cervical Radiculopathy: A Review. HSS journal, 2011. 7: 265 - 272. LoE: 2A
- ↑ Heckmann J, Lang J, Zobelein I, et al. Herniated cervical intervertebral discs with radiculopathy: an issue written report of conservatively or surgically treated patients. J Spinal Disord. 1999;12:396-401.
- ↑ 26.0 26.i 26.ii Cheng CH, Tsai LC, Chung HC, Hsu WL, Wang SF, Wang JL, Lai DM, Chien A. Practise training for not-operative and post-operative patient with cervical radiculopathy: a literature review. 2015 Sep. J Phys Ther Sci. 27(9): 3011-8.
- ↑ 27.0 27.1 Leveque JC. Diagnosis and treatment of Cervical Radiculopathy and Myelopathy. 2015. Physical medicine and rehabilitation clinics of North America 26(3): 491-511.
- ↑ 28.0 28.1 28.two Matz PG1 et al., Indications for inductive cervical decompression for the treatment of cervical degenerative radiculopathy, J Neurosurg Spine. 2009 Aug;xi(ii):174-82. LoE: 2A
- ↑ 29.0 29.1 Engquist Thousand et al., Surgery Versus Nonsurgical Treatment of Cervical Radiculopathy: A Prospective, Randomized Study Comparison Surgery Plus Physiotherapy With Physiotherapy Alone With a 2-Twelvemonth Follow-up. 15 september 2013. Spine, 38(20): 1715–1722.
- ↑ Peolsson A et al. Concrete Function Upshot in Cervical Radiculopathy Patients Later Physiotherapy Lone Compared With Anterior Surgery Followed past Physiotherapy: A Prospective Randomized Study With a two-Yr Follow-up. 15 February 2013. Spine 38(4): 300-307
- ↑ Kim H, Lee SH, Kim MH. Multislice CT fluoroscopy-assisted cervical transforaminal injection of steroids: technical note. J Spinal Disord Tech 2007;20:456–61.
- ↑ Anderberg Fifty, Annertz M, Persson L, et al. Transforaminal steroid injections for the treatment of cervical radiculopathy: a prospective and randomised report. Eur Spine J 2007;16:321–viii
- ↑ Lee SH et al. Clinical Outcomes of Cervical Radiculopathy Following Epidural Steroid Injection: A Prospective Study With Follow-upward for More than Than ii Years. xx May 2012. Spine 37(12): 1041-1047.
- ↑ Boyles, Robert; Toy, Patrick; Mellon, James; Hayes, Margaret; Hammer, Bradley.Effectiveness of manual physical therapy in the treatment of cervical radiculopathy: a systematic review Journal of Manual and Manipulative Therapy 19 (2011) 135-142.
- ↑ Elmasry S, Asfour Due south, de Rivero Vaccari JP, Travascio F. Furnishings of Tobacco Smoking on the Degeneration of the Intervertebral Disc: A Finite Element Report. PLoS One. 2015 Aug 24;10(8):e0136137. LoE: 4
- ↑ 37.0 37.1 Langevin P, Desmeules F, Lamothe M, Robitaille S, Roy JS. Comparison of 2 manual therapy and practise protocols for cervical radiculopathy: a randomized clinical trial evaluating brusque-term effects. 2015 Jan. J Orthop Sports Phys Ther 45(one):4-17.
- ↑ 38.0 38.1 Young IA. et al. Reliability, Construct Validity, and Responsiveness of the Neck Inability Index, Patient-Specific Functional Scale, and Numeric Pain Rating Scale in Patients with Cervical Radiculopathy. American Journal of Physical Medicine & Rehabilitation. Oct 2010; 89(x): 831-839
- ↑ Fredin 1000, Lorås H, Transmission therapy, do therapy or combined treatment in the management of adult neck pain – A systematic review and meta-assay, Musculoskeletal Science and Practice, Volume 31, October 2017, Pages 62-71
- ↑ Anita AR et al. A Cochrane Review of Manipulation and Mobilization for Mechanical Neck Disorders. Spine. 2004; 29(xiv): 1541-1548
- ↑ Cross KM, Kuenze C, Grindstaff TL, Hertel J.Thoracic spine thrust manipulation improves hurting, range of movement, and cocky-reported office in patients with mechanical neck pain: a systematic review.J Orthop Sports Phys Ther. 2011 Sep;41(ix):633-42.
- ↑ Rushton A, Rivett D, Carlesso 50, Flynn T, Hing W, Kerry R. International Framework for Examination of the Cervical Region http://www.physio-pedia.com/Section_5:_Physical_examination
- ↑ Fritz JM, Thackeray A, Brennan GP, Childs JD.Exercise only, do with mechanical traction, or exercise with over-door traction for patients with cervical radiculopathy, with or without consideration of status on a previously described subgrouping rule: a randomized clinical trial. J Orthop Sports Phys Ther. 2014 Feb;44(2):45-57.
- ↑ Jellad A, Ben Salah Z, Boudokhane S, Migaou H, Bahri I, Rejeb N.The value of intermittent cervical traction in contempo cervical radiculopathy.Ann Phys Rehabil Med. 2009 November;52(9):638-52.
- ↑ Boyles R. Toy P. Mellon J. Hayes K.Hammer B. Effectiveness of manual concrete therapy in the treatment of cervical radiculopathy a systematic review. Journal of Manipulative therapy. nineteen (3) 2011
- ↑ 46.0 46.1 Ragonese J. A randomized trial comparing transmission concrete therapy to therapeutic exercises, to a combination of therapies,for the treatment of cervical radiculopathy. Orthop Prac 2009;21(3):71–7.
- ↑ 47.0 47.1 Cleland JA, Whitman JM, Fritz JM, Palmer JA. Manual physical therapy, cervical traction, and strengthening exercises in patients with cervical radiculopathy: a case series. J Ortho Sports Phys Ther 2005;35:802–xi.
- ↑ Franke H, Fryer Yard, Ostelo RW, Kamper SJ .Muscle energy technique for non-specific low-back pain. Cochrane Database Syst Rev. 2015 Feb 27;2:CD009852. LoE: 1A.
- ↑ Butler, 0 (1991). Mobilisation of the Nervous System, Churchill Livingstone, Edinburgh
- ↑ Magee DJ. Orthopedic concrete assessment. 5th ed. St. Louis,MO: Saunders Elsevier; 2008.
- ↑ Malanga G. Sherwin SW.Cervical Radiculopathy Treatment & Management 2013 [ONLINE]fckLRAvailable from http://emedicine.medscape.com/article/94118-treatment#aw2aab6b6b2
- ↑ Griffiths C, Dziedzic Yard, Waterfield J, Sim J. Effectiveness of specific cervix stabilization exercises or a general cervix exercise programme for chronic neck disorders: a randomized controlled trial. J Rheumatol. Feb 2009;36(2):390-7
- ↑ Falla D, Lindstrøm R, Rechter 50, Boudreau S, Petzke F. Effectiveness of an viii-week exercise plan on pain and specificity of neck muscle activity in patients with chronic neck pain: a randomized controlled study. Eur J Pain. 2013; 17: 1517– 1528. LoE: 1B
- ↑ Cleland JA, Fritz JM, Whitman JM, et al. Predictors of curt-term outcomes in people with a clinical diagnosis of cervical radiculopathy. Phys Ther. 2007;87(12):1619-1632.
- ↑ Partanen J, Partanen K, Oikarinen H, et al. Preoperative electroneuromyography and myelography in cervical root compression. Electromyogr Clin Neurophysiol. 1991; 31:21-26.
Source: https://www.physio-pedia.com/Cervical_Radiculopathy
0 Response to "what can you do to relieve the pain of cervical radiculopathy that is compressing the ulnar nerve"
Post a Comment